5 Key Strategies to Enhance Clinical Documentation and Improve Reimbursements
Revenue Cycle Management for Urology: Best Practices for Accurate Coding and Increased Efficiency
November 12, 2024
The Impact of Telehealth on Billing Practices in Specialty Care
November 12, 2024
Are you a healthcare provider investing countless hours into patient care? Yet, are you facing delayed, or denied claims? You are not alone! This scenario is too common among practitioners, and clinical documentation is often overlooked, but a significant factor contributing to this financial loss.
According to the Optum 2024 Revenue Cycle Denials Index, denial rates have increased from 10% in 2020 to 12% in 2024. Of these denials, 12.08% are due to documentation issues that are avoidable. Improper documentation leads to payment delays and denials, leading to financial instability. Additionally, it also impacts the time and resources that could otherwise be spent on patient care.
If you are a healthcare provider looking for ways to improve your documentation practices to improve your reimbursement rates, this blog is for you.
Understanding Clinical Documentation
Clinical documentation is the process of recording patient information in a medical chart or Electronic Health Record (EHR). Quality documentation serves many critical purposes, as it contains up-to-date information on every specific treatment that is provided to the patient, enabling effective treatments in the future.
Clinical documentation also ensures that you are HIPAA compliant and is proof that you have offered appropriate treatment. It can support your practice’s authenticity in case of any claims or lawsuits. It contains:
- Patient history: Medical and family history, allergies, and current medications
- Physical examination: Findings from a physical examination of the patient, like vitals, general appearance, and initial examination
- Diagnosis: The patient’s diagnosis or suspected diagnosis
- Treatment plan: The course of treatment prescribed for the patient, including medications, procedures, and referrals
- Progress notes: The patient’s progress throughout the treatment
The Importance of Clinical Documentation
Clinical documentation is the foundation for the entire revenue cycle management, from coding and billing to reimbursements. Inaccurate and incomplete documentation can lead to claim denials, delays in payments, and increases the risk of audits, impacting a practice’s financial credibility. According to a study, healthcare providers spend over $118 per claim on reworking denied claims.
Quality clinical documentation helps in:
- Proof of appropriate treatment: By clearly documenting the patient’s conditions, diagnosis, and treatment plan, healthcare providers can showcase that the services provided were necessary and appropriate.
- Preventing claim denials: Accurate coding and documentation can help avoid claims denials due to missing or inaccurate information.
- Improving coding accuracy: Detailed and well-organized documentation helps coders to assign correct codes to services, reducing the chances for coding errors.
- Supports audits: In case of an audit, accurate and complete documentation can help support the medical necessity and avoid penalties.
Proper clinical documentation can help healthcare providers improve the reimbursement rates, reduce their administrative burden of having to submit reclaims, and ultimately improve their financial health of the practices.
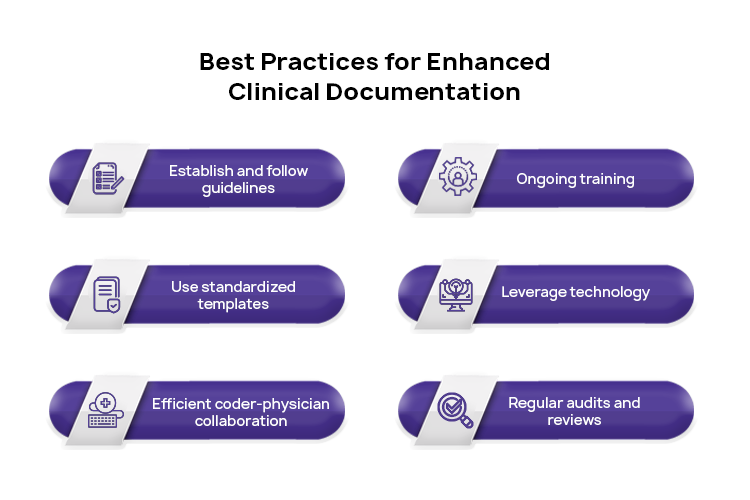
Key Strategies for Enhanced Clinical Documentation
Each healthcare provider has their own method for clinical documentation, and it keeps adapting and evolving as the industry advances. However, providers often deal with documentation errors, such as missing information, misspelt terms and abbreviations, inaccurate visit time calculations, etc.
Quality documentation is crucial to preventing claim denials and ensuring that providers are fairly compensated for their services. Here are some key strategies for healthcare providers to maximize their revenue with quality clinical documentation.
1. Detailed Patient Assessments
Conduct thorough and systematic patient assessment that includes detailed medical histories, current health status, and other relevant medical information. All patient interactions, diagnoses, and treatment plans should be accurately documented.
The documentation should follow the guidelines for E/M services as per the CPT code book. Use standardized templates to ensure that all relevant information is captured consistently across patient records.
2. Detailed Procedure Descriptions
Ensure that all procedures performed are documented in detail with all the specifics. This should include the indications of circumstances that led to the procedure, the technique used, and any sudden complications that arose during the procedure.
Such detailed documentation not only helps in effective coding but also justifies the necessity of performing that procedure. Use standardized language and terminology that aligns with coding guidelines to maintain consistency.
3. Regular Employee Training
Implement regular training sessions for your clinical staff on the importance of quality documentation and updates on coding changes and guidelines. Continuous education ensures that all team members are educated on how to maintain best practices in documentation.
Create an internal documentation manual that can serve as a reference guide for best practices and updates.
4. Leverage Technology
Effectively utilize technological solutions, like Electronic Health Record (EHR) systems, that aid in accurate and efficient documentation. EHRs can provide documentation prompts and templates that ensure that all information is accurately documented.
EHR features like voice recognition and natural language processing can streamline the documentation process and maintain accuracy.
5. Audit and Feedback Mechanisms
Establish a system for auditing clinical documentation and providing feedback to providers. Regular audits help identify areas for improvement and ensure compliance with documentation standards. Use audit results to identify problematic areas and craft training programs that address these issues.
Benefits of Enhanced Clinical Documentation for Reimbursements
By implementing these strategies, healthcare providers can improve their reimbursements and optimize their overall revenue cycle management. Enhanced documentation leads to:
- Fewer claim denials: With accurate and detailed documentation, the chances of claim denials are reduced.
- Improved coding accuracy: Comprehensive documentation ensures that coders have all the information needed to assign appropriate codes, improving the reimbursement potential.
- Quick payment turnaround: Claims supported by quality clinical documentation are processed faster, resulting in faster reimbursements from insurers.
Maximize Reimbursements with Atlantic RCM
Enhanced clinical documentation is crucial not just for improving patient care and compliance, but also for optimizing your financial health. Atlantic RCM can help you improve your reimbursement rates, reduce the administrative burden, and optimize your overall revenue cycle management.
Contact Atlantic RCM today to learn more about how we can help you maximize your reimbursements through enhanced clinical documentation.
Atlantic RCM is one of the leading multi-specialty medical billing companies in USA that serves 25+ major medical billing specialties. Our experts work across your practice in billing, collections and account receivables management, to help you succeed.
Get in touch with the leading medical billing outsourcing company to learn more. Call us at (469) 501-1500 or write to us Info@atlanticrcm.com


{kind=link}
{kind=link}
{kind=link}